Article Text

Abstract
Aims There are limited data on programmed death ligand 1 (PD-L1) expression in oesophageal cancer (OC) from multicentre studies conducted across China. We aimed to determine the prevalence of high PD-L1 expression in patients with advanced OC.
Methods The EXCEED study was a multicentre, retrospective analysis of data from six tertiary hospitals that evaluated PD-L1 expression in adults with advanced OC or advanced head and neck squamous cell carcinoma. PD-L1 expression was evaluated at each site according to a standardised protocol. The primary outcome was the prevalence of high PD-L1 expression (Combined Positive Score (CPS) ≥10) in surgical or tumour biopsy samples. Low PD-L1 expression was defined as CPS <10. Patient demographic and baseline factors associated with high PD-L1 expression were also investigated. This report presents the results for the OC cohort only.
Results Overall, 482 patients were included, the majority were male (87.6%) and the mean age at diagnosis was 63.3 years; 207 had high PD-L1 expression (42.9%; 95% CI 38.5, 47.5) and 275 had low expression (57.1%; 95% CI 52.5, 61.5). There were significant differences in high PD-L1 expression prevalence between subgroups by sex (p=0.044), number of distant metastases (p=0.020), and if chemotherapy (p=0.004) was received prior to the collection of biological samples (ie, biopsy or surgery).
Conclusions These real-world data provide a robust estimate of the prevalence of high PD-L1 expression in patients with advanced OC and identify clinicopathological and treatment features related to PD-L1 expression that can inform treatment selection.
- Esophagus
- NEOPLASMS
- Pathology, Molecular
Data availability statement
Data are available upon reasonable request. Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA (MSD), is committed to providing qualified scientific researchers access to anonymised data and clinical study reports from the company’s clinical trials for the purpose of conducting legitimate scientific research. MSD is also obligated to protect the rights and privacy of trial participants and, as such, has a procedure in place for evaluating and fulfilling requests for sharing company clinical trial data with qualified external scientific researchers. The MSD data sharing website (available at: http://engagezone.msd.com/ds_documentation.php) outlines the process and requirements for submitting a data request. Applications will be promptly assessed for completeness and policy compliance. Feasible requests will be reviewed by a committee of MSD subject matter experts to assess the scientific validity of the request and the qualifications of the requestors. In line with data privacy legislation, submitters of approved requests must enter into a standard data-sharing agreement with MSD before data access is granted. Data will be made available for request after product approval in the USA and EU or after product development is discontinued. There are circumstances that may prevent MSD from sharing requested data, including country or region-specific regulations. If the request is declined, it will be communicated to the investigator. Access to genetic or exploratory biomarker data requires a detailed, hypothesis-driven statistical analysis plan that is collaboratively developed by the requestor and MSD subject matter experts; after approval of the statistical analysis plan and execution of a data-sharing agreement, MSD will either perform the proposed analyses and share the results with the requestor or will construct biomarker covariates and add them to a file with clinical data that is uploaded to an analysis portal so that the requestor can perform the proposed analyses.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Immunotherapy is an effective treatment option for patients with advanced oesophageal cancer (OC), and programmed death ligand 1 (PD-L1) expression can predict outcomes to immunotherapy.
However, data on PD-L1 expression show high variability due to heterogeneous testing methodologies and geographical/regional differences due to genetic, environmental and other factors.
WHAT THIS STUDY ADDS
The results of the multicentre EXCEED study provide real-world estimates of PD-L1 expression status in patients with advanced oesophageal squamous cell carcinoma.
PD-L1 expression was evaluated consistently across all patients using unified standards and training, which limited intra-study variability and provides a robust and pertinent dataset.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The findings of this study will inform patient selection for immunotherapy and support clinical decision-making during the ongoing development of precision medicine for the treatment of advanced OC.
Introduction
Oesophageal cancer (OC) is the ninth most common cancer worldwide and sixth most frequent cause of cancer-related death globally.1 China accounts for >50% of global total new cases of OC, with an incidence rate at least five times higher than any other country.2 OC is classified as either squamous cell carcinoma (OSCC) or adenocarcinoma (OAC); these subtypes differ in characteristics, treatment strategies and prognosis.3 There are also geographical differences in the distribution of OC subtypes globally due to specific risk factors between regions; for example, OSCC accounts for around 90% of new OC cases in China vs 30–40% in Western countries.4 5 OC often presents with non-specific symptoms or remains asymptomatic in early stages, leading to delayed diagnosis, meaning advanced disease at time of presentation is common.2 6 7 As a result, the prognosis for OC is generally poor, especially for advanced stages (III and IV). Metastatic OC is associated with a particularly poor prognosis, with a 5-year survival rate of <5%.7
The US National Comprehensive Cancer Network (NCCN) guidelines recommend a tailored treatment approach for OC, based on factors including histological type, disease stage and patient characteristics.8 Recommended therapies for advanced OC include chemotherapy, chemoradiotherapy and targeted therapies such as human epidermal growth factor receptor 2 (HER2) inhibitors and programmed cell death protein-1 (PD-1) or programmed cell death ligand-1 (PD-L1) inhibitors in patients with specific molecular aberrations.8 9 Immunotherapy with immune checkpoint inhibitors (ICIs) targeting the programmed cell death pathway, including PD-1 and PD-L1, has emerged as a promising treatment modality in OC.9–11 PD-1/PD-L1 inhibitors have demonstrated significant value in advanced OC, providing durable responses and survival rates.9 12 ICIs enhance the ability of the immune system to recognise and eliminate cancer cells in the tumour microenvironment where PD-L1 expression is often upregulated as an immune evasion strategy.13 By restoring T-cell activity, PD-1/PD-L1 inhibitors can lead to tumour regression and prolonged survival.13
PD-L1 expression is a potential predictive biomarker for efficacy of PD-1/PD-L1 inhibitors and may therefore enable identification of patients more likely to benefit from these agents.13 14 However, available data on PD-L1 expression show high inter-study and intra-study variation, likely due to differences in study populations and methodologies, antibody clones used for PD-L1 assessment and cut-off values for defining positive expression.12 Standardised PD-L1 testing methods, including antibody selection, staining platforms and scoring systems, are still being established to ensure consistent, reliable assessments of PD-L1 expression. Studies have also identified geographical variation in PD-L1 expression, for example, Asian populations have shown relatively high PD-L1 expression rates versus Western populations.15 16 Such regional differences in PD-L1 expression could be influenced by genetic, environmental or other factors.
PD-L1 expression is relatively common in OSCC, with studies in Chinese populations reporting prevalence rates up to 80%.17 18 However, further research is needed to better understand the prevalence of PD-L1 expression in OC across patient populations and explore its potential as a predictive biomarker for response to PD-1/PD-L1 inhibitors. Determination of PD-L1 expression prevalence in OC will contribute to the development of precision medicine and inform patient selection and treatment decision-making for OC. The present study aimed to determine the prevalence of high PD-L1 expression in patients with advanced OC.
Materials and methods
Study design
The EXCEED study was a nationwide, multicentre, retrospective analysis of data from six tertiary (Tier 3) hospitals in Beijing, Zhengzhou, Wuhan, Guangzhou, Shanghai and Chengdu, evaluating PD-L1 expression in patients with advanced OC or advanced head and neck squamous cell carcinoma (HNSCC). Participants were screened and enrolled between 9 August 2021 and 28 February 2022. The current report presents results for the OC cohort only.
The study was conducted in accordance with the Declaration of Helsinki and informed consent was obtained from all patients before enrolment. The protocol was approved by independent ethics committees at each study site prior to study initiation. The study was registered at the ISRCTN registry (#ISRCTN 10570964).
Patient involvement
Patients were not involved in the design and conduct of this research.
Participants
Eligible patients were aged ≥18 years at OC diagnosis and had locally advanced and unresectable, or metastatic, histologically confirmed adenocarcinoma or squamous cell carcinoma of the oesophagus or Siewert type I adenocarcinoma of the oesophageal-gastric junction (OGJ, defined as adenocarcinomas of the lower oesophagus with the centre located 1–5 cm above the anatomic OGJ). Patients were required to have an available formalin-fixed, paraffin-embedded surgical or biopsy specimen. Samples could be either newly obtained (ie, collected ≤6 weeks prior to PD-L1 test) or archival (>6 weeks but ≤1 year old) specimens acquired from primary tumour or metastatic sites, with newly obtained, primary tumour samples preferred. Patients with fine-needle aspirates or cytologic specimens were excluded.
Outcomes
The primary outcome of this analysis was the prevalence of high PD-L1 expression, defined as a Combined Positive Score (CPS) ≥10, in patients with advanced OC. Low PD-L1 expression was defined as CPS <10. Patient demographic and baseline factors associated with high PD-L1 expression were investigated as secondary outcomes.
Study variables
Patient data were collected from electronic medical record systems or, if unavailable, by chart review. Study variables included demographics (age at diagnosis, sex, family history of EC, and smoking/alcohol consumption history), clinicopathological parameters (tumour stage, Eastern Cooperative Oncology Group performance status (ECOG PS), histology, grade, number/location of metastases and biopsy site/type), prior OC treatment status (including systemic/targeted therapies), and biomarkers other than PD-L1 (HER2 and epidermal growth factor receptor (EGFR) expression,19 20 microsatellite instability-high (MSI-H, chromosome level abnormality measured by PCR) and/or deficient mismatch repair (dMMR, protein level measured by immunohistochemistry) status and tumour mutational burden (TMB)), when available.
PD-L1 measurement
PD-L1 expression was evaluated at each site according to a standardised protocol. For each specimen, at least three 4 µm sections, freshly cut within 1 month of assay (preferably within 1 week), were required: one for PD-L1 testing, one as PD-L1 negative control and one for H&E staining to assess tissue histology and preservation quality. PD-L1 expression was evaluated according to the manufacturer’s instructions using the qualitative PD-L1 immunohistochemistry (IHC) 22C3 pharmDx assay with the EnVision FLEX visualisation system on the Dako Autostainer Link 48 platform (Agilent Technologies, Santa Clara, California, USA). The level of immunostaining was assessed based on CPS, calculated by dividing the number of PD-L1 staining cells (ie, tumour cells, lymphocytes and macrophages) by the total number of viable tumour cells and multiplying the result by 100. Lymphocytes and macrophages (mononuclear inflammatory cells) present within tumour nests and/or adjacent supporting stroma (at a ×20 magnification, ie, within 0.5 mm of the tumour cells) were considered directly associated with tumour response (tumor-associated) and included in the CPS numerator. This rule was also applied to lymph node metastasis.21 Both IHC assay and CPS scoring were performed locally by pathologists trained and certified in these assessments by the sponsor. All local laboratories were pathology units at tertiary hospitals with either prior experience of similar research and/or willingness to collaborate with the sponsor to ensure optimal sample storage and access to the platform.
Statistical analyses
The sample size calculation assumed a prevalence of high PD-L1 expression in patients with advanced OC of 44%, based on the Chinese subgroup of KEYNOTE-181.22 A total of 396 evaluable samples would be required to estimate prevalence with a precision level of ±5% for the 95% CI. Accounting for a non-evaluable sample rate of 14%, as seen in a similarly designed study evaluating PD-L1 expression in Chinese patients with non-small cell lung cancer (NSCLC),23 the final planned sample size was 460 patients.
The prevalence of high PD-L1 expression was expressed as percentage, with the associated 95% Clopper-Pearson interval, for patients with available CPS data. Prevalence was compared between patient subgroups defined according to demographic and clinicopathological characteristics, prior treatment status and other biomarkers, using the χ2 test or Fisher’s exact test for categorical variables when expected frequencies were <5, or the Wilcoxon rank-sum test for ordinal variables. Univariate logistic regression was used to estimate OR, with associated 95% CI and p values, for pairwise comparisons of prevalence between subgroups for each variable. Subgroup analyses included only patients with available data for each variable analysed. P values <0.05 were considered statistically significant.
Statistical analyses were performed using SAS V.9.4 (SAS Institute). The date of final clinical database lock was 18 August 2022.
Results
Patients
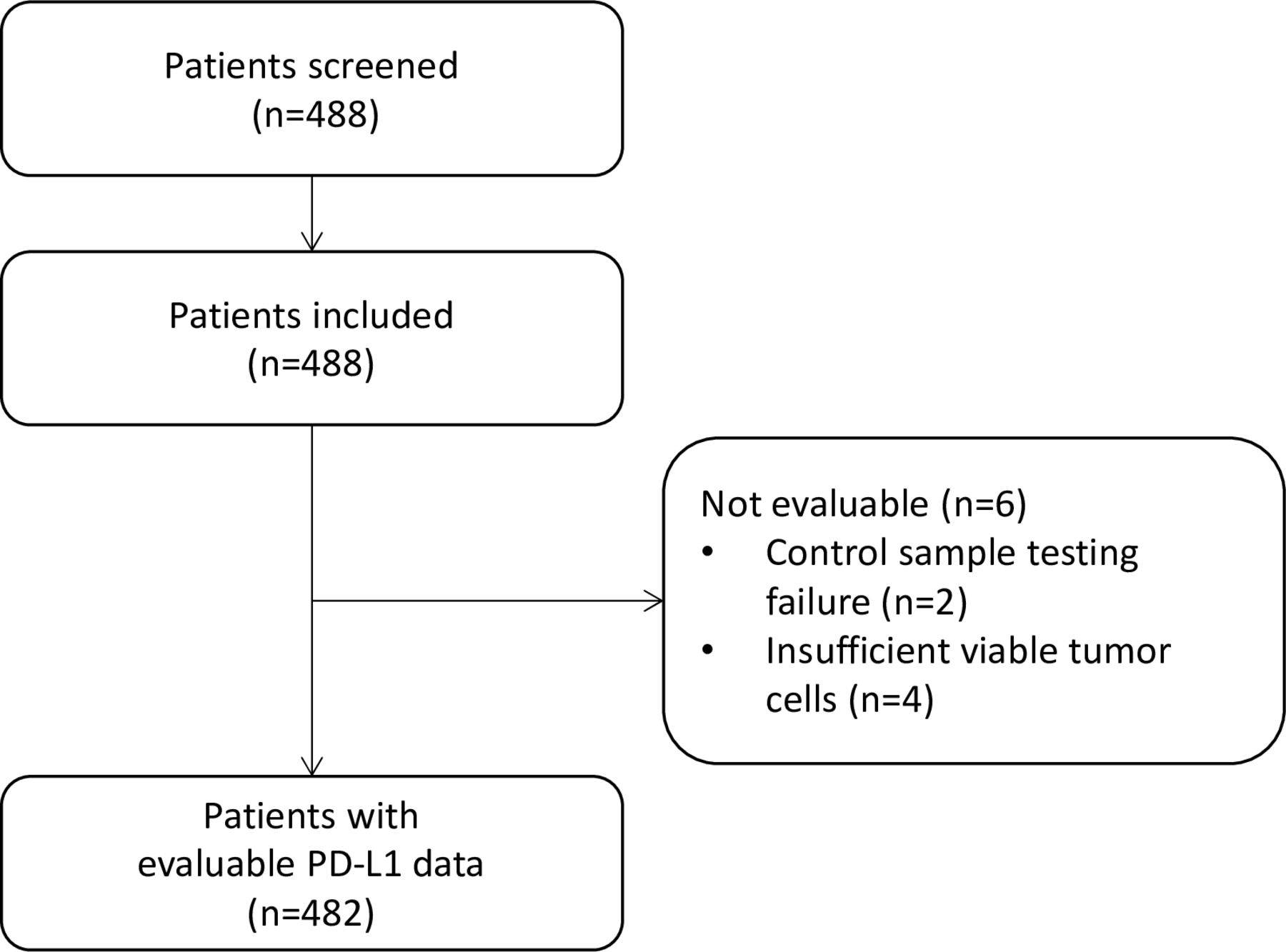
Overall, 488 patients with OC were screened, enrolled and provided tumour tissue specimens (figure 1). Samples from six patients were not evaluable for PD-L1 expression due to insufficient viable tumour cells (n=4) or failure of control sample testing (n=2), meaning 482 patients were included in the final analysis. The majority were male (n=422; 87.6%) and mean age at diagnosis was 63.3 years (SD 8.2) (table 1). A total of 307 patients (63.7%) had no family history of OC, 185 (38.4%) were non-smokers and 224 (46.5%) abstained from alcohol. The most common systemic/targeted treatments received prior to inclusion (and prior to collection of biological samples) were chemotherapy (n=135; 28.0%), immunotherapy (n=26; 5.4%) and radiotherapy (n=24; 5.0%).

Patient selection process. PD-L1, programmed death ligand-1.
Patient demographics and baseline characteristics
Tumour histology was OSCC in the vast majority of patients (n=478; 99.4%); most had poorly (n=159; 33.1%) or moderately (n=235; 48.9%) differentiated tumours.
Tumour samples and biomarker measurements
Tumour tissue samples were mostly archival specimens (n=463; 96.1%). The majority of samples were collected from the primary tumour (n=476; 98.8%), three (0.6%) from lymph nodes and three (0.6%) decalcified bone lesion specimens (table 2). Tumour tissue was obtained via surgery in 344 patients (71.4%) and biopsy in 138 (28.6%).
Summary of specimen preparation
HER2 and EGFR IHC expression scores were available for 69 and 15 patients, respectively. Among these subgroups, the HER2 IHC score was 0 in 51 patients (73.9%), 1+ in 12 patients (17.4%), 2+ in five patients (7.2%) and 3+ in one patient (1.4%), while the EGFR IHC score was 0 in one patient (6.7%), 2+ in nine patients (60.0%) and 3+ in five patients (33.3%). Five patients had MSI-H and/or dMMR status: among 11 patients with MSI data, one (9.1%) had MSI-H status, while among 75 patients with MMR data, four (5.3%) had dMMR status. In one patient with available data, the TMB was 3.8 mutations/Mb.
PD-L1 expression
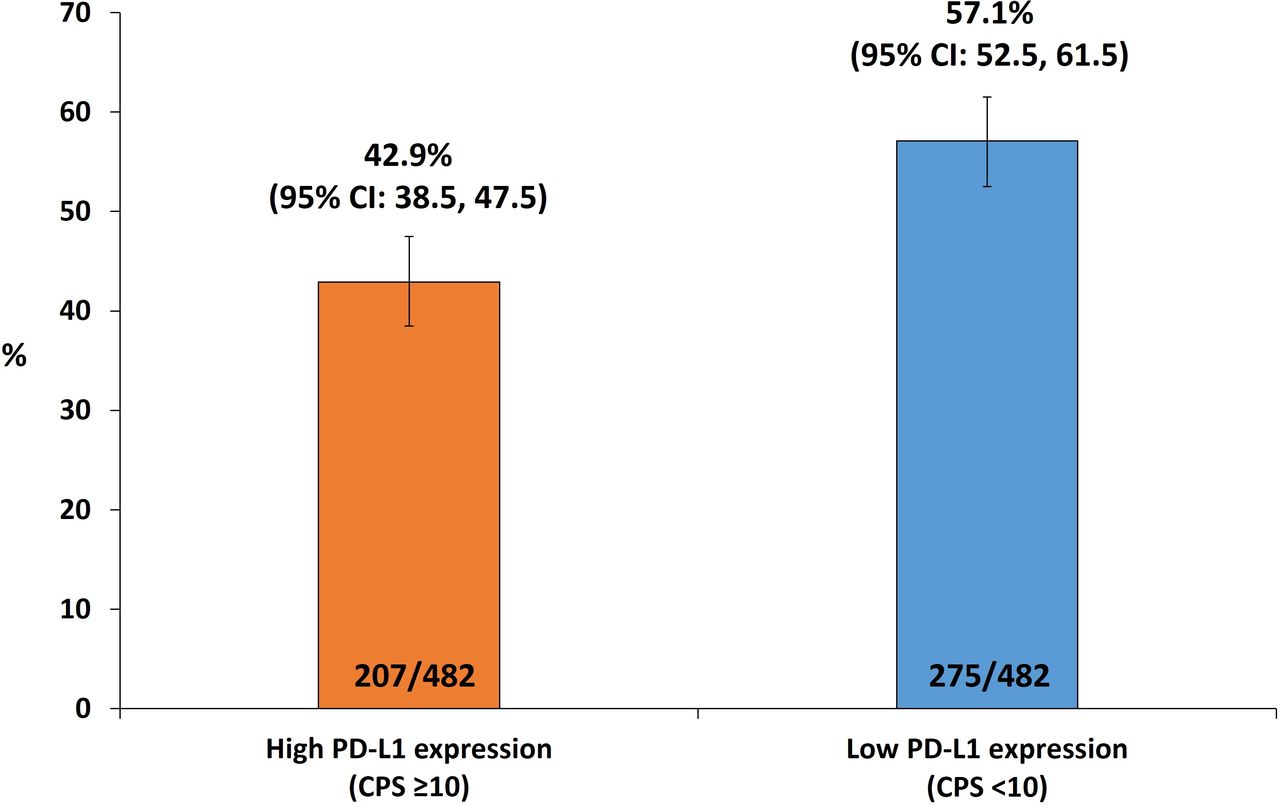
Among 482 patients evaluated, 207 had high PD-L1 expression (42.9%; 95% CI 38.5, 47.5) and 275 had low PD-L1 expression (57.1%; 95% CI 52.5, 61.5; figure 2).

Prevalence of high and low PD-L1 expression in patients with advanced oesophageal cancer. Prevalence was calculated using the total number of patients evaluable for PD-L1 expression as the denominator. High PD-L1 expression was defined as CPS ≥10, low PD-L1 expression was defined as CPS <10. Error bars indicate the 95% Clopper-Pearson interval. CPS, Combined Positive Score; PD-L1, programmed death ligand-1.
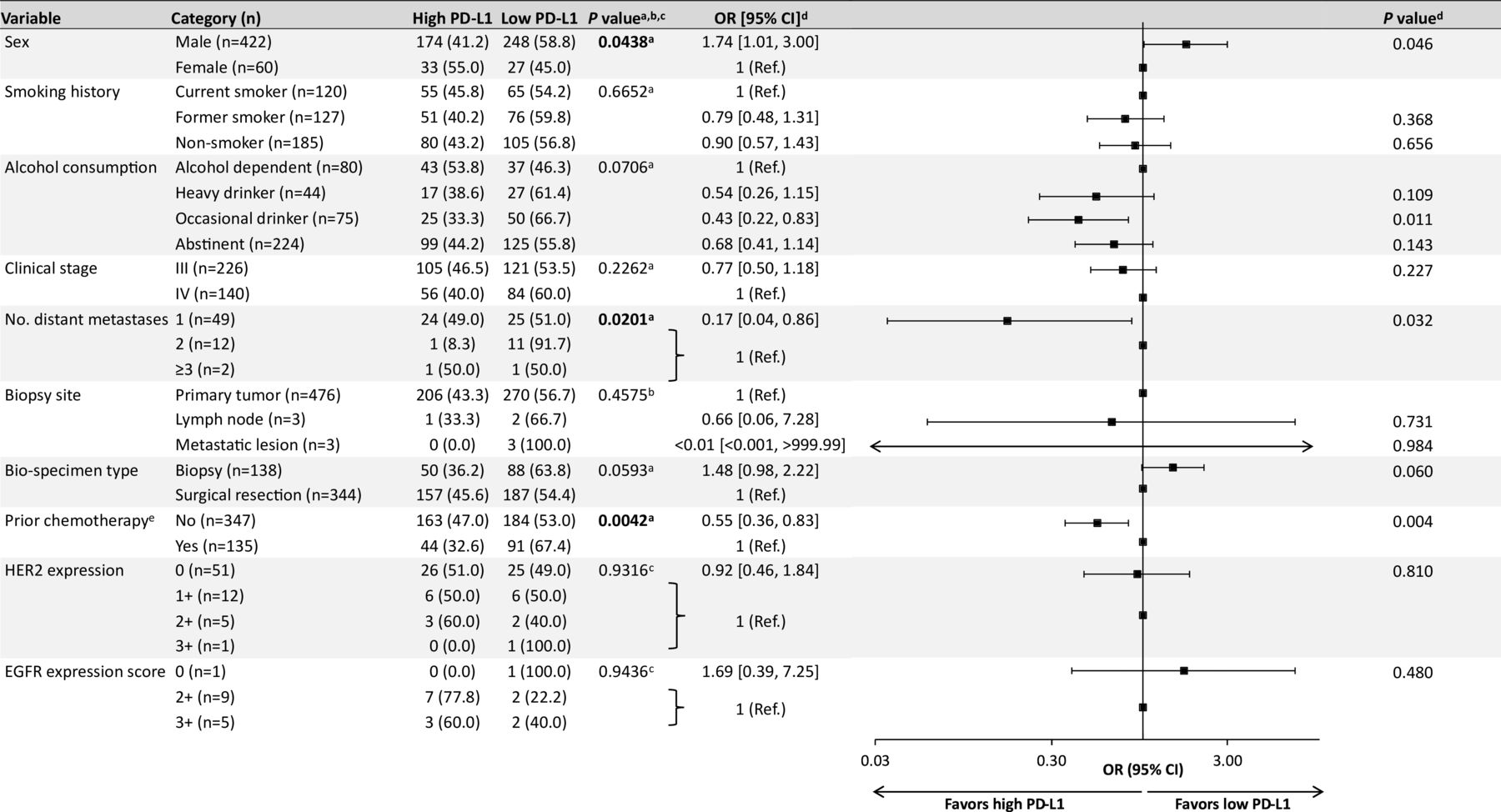
χ2 or Wilcoxon rank-sum tests showed significant differences in the prevalence of high PD-L1 expression between subgroups defined according to sex (p=0.044), distant metastases (p=0.020), and prior chemotherapy (p=0.004; figure 3). In univariate logistic regression analyses, the prevalence of high PD-L1 expression was significantly greater in women versus men (55.0% vs 41.2%; OR 1.74; 95% CI 1.01, 3.00; p=0.046). Conversely, there was a lower prevalence of high PD-L1 expression in occasional drinkers versus patients with alcohol dependency (33.3% vs 53.8%; OR 0.43, 95% CI 0.22, 0.83; p=0.011), patients with ≥2 vs 1 distant metastatic lesion (14.3% vs 49.0%; OR 0.17; 95% CI 0.04, 0.86; p=0.032) and history of chemotherapy prior to sample collection versus no prior chemotherapy (32.6% vs 47.0%; OR 0.55; 95% CI 0.36, 0.83; p=0.004). PD-L1 high prevalence was comparable in patients with clinical stage III versus stage IV disease (46.5% vs 40.0%; OR 0.77; 95% CI 0.50, 1.18; p=0.2262).

{kind=link}
{kind=link}
{kind=link}
Subgroup analysis of PD-L1 expression. aχ2 test. bFisher’s exact test. cWilcoxon rank-sum test. dUnivariate logistic regression. eReceived prior to the collection of biological samples (ie, biopsy or surgery). EGFR, epidermal growth factor receptor; HER2, human epidermal growth factor receptor-2; OR, odds ratio; PD-L1, programmed death ligand 1; Ref, reference.
Discussion
PD-L1 expression is a predictive biomarker for sensitivity to ICI therapy in patients with OSCC.13 14 Therefore, understanding PD-L1 expression levels is important to guide treatment selection and optimise outcomes. This is particularly pertinent in China where OC represents a major public health concern. The results of the EXCEED study provided real-world estimates of PD-L1 expression in patients with advanced OSCC, among which 207 out of 482 (42.9%) had high PD-L1 expression (CPS ≥10). Data on PD-L1 expression in patients with cancer show high inter-study and intra-study variation.12 In the EXCEED study, PD-L1 expression was evaluated consistently across patients using unified standards and training, which should limit intra-study variability and provide a robust and pertinent dataset to inform future investigations.
Our findings support those from a previous single-centre study of samples from 533 patients with OC in China, which reported high PD-L1 expression in 226 out of 483 (46.8%) patients with OSCC.24 The results are also consistent with the Asia-specific analysis (excluding China), and the Chinese extension arm, of the phase 3 KEYNOTE-181 clinical trial, which investigated pembrolizumab versus chemotherapy in patients with OSCC with high PD-L1 expression (CPS ≥10).22 This study reported CPS ≥10 in 57 out of 110 (51.8%) and 54 out of 111 (48.6%) patients receiving pembrolizumab or chemotherapy, respectively, in the Asian subgroup and 24 out of 60 (40.0%) and 28 out of 59 (47.5%) in the China cohort.22 A Chinese subgroup analysis of KEYNOTE-590, including 98% of patients with OSCC, reported high PD-L1 expression in 52 out of 106 (49.1%) patients.25
In contrast with the findings of the present study, in the global analysis of the KEYNOTE-181 study, 222 out of 628 (35.4%) patients with recurrent locally advanced/metastatic OC had high PD-L1 expression.26 Similarly, in the global cohort of KEYNOTE-590, there was a lower incidence of high PD-L1 expression in patients with OSCC (286/749; 38.2%) compared with the present study.27 Racial differences in PD-L1 expression may explain the distinction between reports, since higher expression is seen in Asian populations. In addition, since OSCC is less common in Western versus Asian countries,4 a high prevalence of OAC among global study populations may also have contributed to the differences observed versus the present study. It is therefore important to consider how geographical variability in PD-L1 expression may influence the antitumour activity of ICIs for OC, as observed in other cancer subtypes.28
The results of the EXCEED study found that PD-L1 expression in advanced OC was influenced by baseline demographics including sex and alcohol consumption, clinicopathological characteristics such as number of distant metastatic lesions, and chemotherapy received prior to biological sample collection (ie, biopsy/surgery). Specifically, higher PD-L1 expression was observed in female patients, patients with alcohol dependency, individuals with only one distant metastatic lesion and those with no prior chemotherapy. Together, these data highlight several patient populations who may benefit from PD-1/PD-L1 inhibitors and suggest avenues for future research into biomarkers for PD-1/PD-L1 inhibitors.
There have been few previous reports of an association between PD-L1 expression and sex in OSCC. However, multiple studies have highlighted a male predominance in oesophageal and gastric cancers, identified associations between genetic variants in sex hormone metabolic genes and OSCC risk, and suggested an impact of sex on treatment responses and survival outcomes.29–35 Specifically, the incidence of oesophageal and gastric cancers was higher in males versus females globally from 2003 to 2012.32 A Chinese study suggested a potential link between sex hormone metabolism genes and OSCC risk, revealing significant associations with individual genes but no overall pathway-level associations.34 Furthermore, multiple studies of neoadjuvant chemoradiotherapy have shown better outcomes in female versus male patients with OSCC, suggesting sex is associated with treatment outcomes and may be due to sex-related differences in drug metabolism.30 31 33 A further study suggested differences in body structure may also impact treatment outcomes in OSCC.29 However, in contrast to the present results, data in gastric cancer and nasopharyngeal cancer have shown no association between PD-L1 expression and sex.36 37
Chemotherapy is known to modulate the tumour immune microenvironment,36 38 39 mediated directly through the immunostimulatory effect of killing cancer cells and through off-target effects on immune cells.40 However, the immunosensitising effect of chemotherapy is related to chemotherapy dose; higher doses of chemotherapy can cause immunosuppression.40–42 Data on the association between chemotherapy use and PD-L1 expression in OSCC are equivocal and appear to depend on treatment regimen. For example, studies have shown a reduction in PD-L1 expression post-chemoradiation,43 while others have shown an increase.39 Similarly, neoadjuvant chemotherapy has been shown to decrease PD-L1 expression in some studies,38 39 including an analysis of paired OSCC tumour samples pre- and post-chemotherapy,44 while it led to an increase in PD-L1 expression in studies conducted in Hong Kong18 and Japan.45 A further study found that PD-L1 expression in OSCC was influenced by preoperative chemotherapy, but PD-L1/L2 expression in primary lesions did not consistently match that of metastatic or recurrent lesions.46 Studies in breast cancer and NSCLC have also found low concordance in PD-L1 expression between primary and metastatic tumours, potentially due to changes in the immune microenvironment of tumours over the disease course.47 48 A 2020 Chinese Expert consensus on standards of PD-L1 testing in NSCLC also concluded that while chemotherapy and chemoradiotherapy modulate PD-L1 expression, no clear trends can be observed in the available data.49 High tumour burden can also negatively affect antitumor immunity, perhaps explaining why patients in the present study with only one distant metastatic lesion had higher PD-L1 expression.50 Together, changes in tumour PD-L1 expression that can occur over the disease course add to the complexity of PD-L1 expression analyses, and a single evaluation of PD-L1/L2 expression may not be sufficient.46–48 Further investigation, for instance, with pairwise sampling, is therefore warranted.
Limitations of this study include the observational nature of the design which could have introduced bias, for example, in the identification of patients as drinkers or smokers. Also, although training in PD-L1 testing was provided to all participating pathologists, some degree of subjective bias in imaging interpretation should be expected. In addition, owing to the previously reported discrepancy between assessments of PD-L1 expression using biopsy and resected specimens in NSCLC and HNSCC, tissue biopsy may have underestimated the expression of PD-L1 in this population.51 52 However, it should be noted that it is often necessary to use biopsy specimens to evaluate PD-L1 expression in patients with advanced, inoperable disease.53 Finally, while the study population included patients from various geographical regions, findings may not be representative of the entire national population of patients with advanced OC. Multivariate analyses are warranted in future studies with larger sample sizes and number of variables.
In summary, this real-world study has determined the prevalence of high PD-L1 (CPS ≥10) expression in patients with advanced OC and identified clinicopathological and treatment features related to PD-L1 expression. These findings can be used to inform patient selection and support clinical decision-making during the ongoing development of precision medicine for the treatment of advanced OC.
Data availability statement
Data are available upon reasonable request. Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA (MSD), is committed to providing qualified scientific researchers access to anonymised data and clinical study reports from the company’s clinical trials for the purpose of conducting legitimate scientific research. MSD is also obligated to protect the rights and privacy of trial participants and, as such, has a procedure in place for evaluating and fulfilling requests for sharing company clinical trial data with qualified external scientific researchers. The MSD data sharing website (available at: http://engagezone.msd.com/ds_documentation.php) outlines the process and requirements for submitting a data request. Applications will be promptly assessed for completeness and policy compliance. Feasible requests will be reviewed by a committee of MSD subject matter experts to assess the scientific validity of the request and the qualifications of the requestors. In line with data privacy legislation, submitters of approved requests must enter into a standard data-sharing agreement with MSD before data access is granted. Data will be made available for request after product approval in the USA and EU or after product development is discontinued. There are circumstances that may prevent MSD from sharing requested data, including country or region-specific regulations. If the request is declined, it will be communicated to the investigator. Access to genetic or exploratory biomarker data requires a detailed, hypothesis-driven statistical analysis plan that is collaboratively developed by the requestor and MSD subject matter experts; after approval of the statistical analysis plan and execution of a data-sharing agreement, MSD will either perform the proposed analyses and share the results with the requestor or will construct biomarker covariates and add them to a file with clinical data that is uploaded to an analysis portal so that the requestor can perform the proposed analyses.
Ethics statements
Patient consent for publication
Ethics approval
The study was conducted in accordance with the principles outlined in the Declaration of Helsinki and informed consent was obtained from all patients before enrolment. The protocol was approved by independent ethics committees at each study site prior to study initiation as follows: Ethics Committee of National Cancer Center/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College (approval no. 20/377-2573), Ethics Committee of Henan Cancer Hospital (approval no. 2020103012-001), Ethics Committee of Tongji Hospital, Tongji Medical College, Huazhong University of Science & Technology (approval no. 2020-S332), Ethics Committee of Sun Yat-Sen University Cancer Center (approval no. B2021-087-01), Ethics Committee of Fudan University Shanghai Cancer Center (approval no. 2102231-16) and Ethics Committee of Biomedical Research, West China Hospital of Sichuan University (approval no. 2021-343). The study was registered at the ISRCTN registry (#ISRCTN 10570964). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
Medical writing support was provided by Jake Burrell, PhD, on behalf of Rude Health Consulting Ltd. This support was funded by MSD China.
References
Footnotes
Handling editor Vikram Deshpande.
Contributors J Yun, LX, J Ying, YL, JQ, YW, WT and JL contributed to conception, design or planning of the study. J Yun, LX, J Ying, LJ, DW, JW, KD, SL, YJ, PD, YW and JL contributed to the acquisition of the data. JY, DW, KD, DH and JL contributed to analysis of the data. J Yun, LX, JQ, YW and JL contributed to interpretation of the results. JL contributed to drafting of the manuscript. All authors contributed to reviewing or revising the manuscript for important intellectual content. J Yun, LJ, SL and YJ contributed to provision of study materials/patients. YW contributed to administrative, logistical or technical support. All authors read and approved the final version of the manuscript. J Yun is the guarantor.
Funding This manuscript was funded by MSD China.
Competing interests JQ, WT and JL are employees of MSD China. YW was formerly an employee of MSD China and is a Takeda shareholder; all other authors have no conflicts of interest to declare.
Provenance and peer review Not commissioned; externally peer reviewed.