Article Text

Abstract
Aims Triple-negative breast cancer (TNBC) is prognostically and therapeutically heterogeneous. The mitotic activity index (MAI) and fibrotic focus (FF) have been established as predictors in non-TNBC but not in TNBC. Late distant metastases occur in TNBC, but previous studies had short follow-up. High stromal tumour-infiltrating lymphocytes (sTILs) are prognostically favourable, but prognostic sTILs-thresholds are not well assessed. We evaluated prognostic/predictive characteristics in an observational population-based cohort of 231 consecutive TNBC patients with long follow-up.
Methods MAI, FF, sTILs and other characteristics were analysed with standard receiver operating characteristic curve analysis, percentile-derived prognostic thresholds, univariate and multivariate survival methods. A TNBC index and decision tree were assessed for distant metastasis-free survival.
Results Long follow-up was decisive: 7% of patients developed late distant metastases. In agreement with the aggressive nature of TNBC, the strongest prognostic MAI-threshold was 5 (p=0.001), lower than that for non-TNBC phenotypes. Lymph-node (LN) status (p=0.0003), FF (p=0.002), MAI5 (p=0.009) and sTILs (threshold 40%, p=0.003) were multivariable based significant and independent prognosticators, but no other characteristics (age, tumour size and grade). LN status was the strongest prognosticator, followed by FF, MAI5 and sTILs40. Subgroup analyses of patients undergoing adjuvant chemotherapy (ACT) showed that only FF and sTILs had significant prognostic value, while LN-positivity and the combination of LN-positivity and MAI≥5 could be a predictive factor for ACT outcome.
Conclusions LN status, MAI5, FF and sTILs40 are prognostic factors in TNBC patients. In TNBC patients who have undergone ACT, the combination of LN-positivity and MAI5 is predictive for response to treatment.
- Breast Neoplasms
- Biomarkers, Tumor
- CARCINOMA
- LYMPHOCYTES
- fibrosis
Data availability statement
Data are available on reasonable request. The dataset generated during the current study is not publicly available because of ethical and legal concerns. Anonymised data can be made available from the Stavanger University Hospital Institutional Data Access/ Ethics Committee (contact via email: rek-vest@uib.no, REK vest, Rogaland, Vestland, Norway) for researchers who meet the criteria for access to confidential data.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Triple-negative breast cancer (TNBC) is a heterogeneous subtype with poor prognosis and limited treatment options. Stromal tumour-infiltrating lymphocytes (sTILs) are a favourable prognostic factor, but there is no consensus on the threshold, and fibrotic focus (FF) is an unfavourable prognostic factor with limited studies in TNBC cohorts.
WHAT THIS STUDY ADDS
This study provides a reliable assessment of prognostic factors, including TNBC-specific thresholds for well-defined sTILs and the mitotic activity index (MAI). The multivariate prognostic TNBC index was designed to classify patients based on their risk of distant metastasis by integrating lymph node status, FF, MAI and sTILs.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The findings may contribute to the use of the TNBC index in clinical practice and future research on personalised treatment strategies.
Introduction
Triple-negative breast cancer (TNBC) is characterised by oestrogen receptor (ER), progesterone receptor (PR) and HER2 negativity. Approximately 15% of all breast cancer (BC) cases in Europe are TNBC; however, much higher percentages (30%–60%) are found in specific populations in the USA and Africa.1–3 TNBC is histologically, prognostically and therapeutically heterogeneous.4–6 As endocrine and anti-HER2 targeted treatments are not options, chemotherapy is the most used treatment. However, its side effects are well known, and TNBC does not always react to chemotherapy. Consequently, TNBC can manifest in a more aggressive manner than other BC phenotypes, and strong prognostic markers are required for optimal clinical care.
Tumour-infiltrating lymphocytes (TILs) have been described in all BC subtypes, and they are most prevalent in TNBC, which makes immunotherapy an option for TNBC.7 Researchers have studied TILs for at least four decades. In 2010, a formal TILs evaluation method was published,7 followed by the International TILs Working Group (TIL-WG) in 2015.8 Studies have shown that TILs scoring methods using H&E-stained slides have acceptable interobserver agreement,9 as such the 2019 St Gallen International Breast Cancer Consensus recommended routine evaluation of TILs in TNBC.10 Currently, the reproducibility of sTILs is still just acceptable, and still no consensus is established regarding the prognostic threshold. These criteria are essential conditions for the use of a pathology laboratory test.11 In fact, studies have described many different prognostic thresholds for stromal TILs (sTILs), such as a 10% incremental threshold,12 three-tier partition,13 four-tier partition14 or two-tier partition with widely different thresholds (eg, 30%,15 50%12 16–18 or even 60%19). This enormous variation may be because most studies involved small cohorts, included lymph node (LN)-negative and/or LN-positive cases, and, above all, short follow-up. Inadequate follow-up is an especially worrisome issue, as distant metastases in TNBCs can occur after one-to-three decades. Therefore, a definitive, prognostically defined threshold for sTILs in TNBC has yet to be determined.
Another stromal component that should be further investigated is fibrotic focus (FF). The literature previously defined BC with FF as a ‘scar cancer’.20 Later studies detailed its cause, definition and prognostic significance.21–24 FF is easily detectable, can vary in size and is usually located at the centre of a tumour.21 25 FF formation is thought to be the result of the hypoxia-induced production of desmoplastic stroma, which consists of fibroblasts, endothelial cells and tumour-associated macrophages.22 These stromal changes may play an important role in tumour cells’ growth, invasive potential and metastasis.26 FF presence is prognostic in BC22 23 27–31 and in three TNBC studies.24 32 33 In one of the TNBC studies (62 patients, 60-month follow-up), FF and/or myxoid changes in the stroma were poor prognostic indicators, and FF presence was significantly associated with low levels of sTILs.32 The other (344 patients, 3–120 months follow-up) evaluated multiomics data, sTILs and FF. The presence of FF was characterised by TGF-ß pathway activation and low sTILs levels.24 The last one (485 patients, median 240-month follow-up) found that the presence of FF was an independent negative prognostic factor in LN-negative early-stage TNBCs.33
Studies with short follow-up are less reliable, especially because TNBCs are prognostically heterogeneous and metastases can occur one-to-three decades later. A short follow-up is an especially serious biasing factor that causes underestimations of the prognostic value of features.
Our aim is to reliably assess the prognostic value of different clinical and pathological factors in TNBC. We conducted an observational study of a large population-based cohort of consecutive TNBC cases, engaging in up to 380 months of follow-up. To assess the prognostic value of the continuous feature sTILs, we used standardised and thoroughly scientifically validated statistical methods.
Materials and methods
This is an observational study, as medicinal products were prescribed in the usual manner in accordance with the terms of marketing authorisation and the effects of risk factors, treatments or other interventions were observed without attempting to change who was or was not exposed to them.34 All patients were treated following the Norwegian Breast Cancer Group national guidelines at the time of diagnosis. We obtained patients’ demographic information, including their date of birth, primary diagnosis, first metastasis, final follow-up and death, treatment modality, and status at follow-up, from the hospital information system.
Patients and histopathological analysis
A total of 284 consecutive TNBC patients diagnosed at Stavanger University Hospital in Norway (1978–2004) were originally considered. We omitted the following cases: 9 cases whose paraffin blocks lacked enough tissue, 29 cases with no LN excision and 15 cases with contralateral BC. This left 231 patients. The specimens were fixed in 4% buffered formaldehyde, dehydrated, embedded in paraffin, cut to 3 µm and stained with H&E. Two expert pathologists (UK and EGG) selected the most representative slide for each patient and evaluated histopathological features (histological type, tumour grade, FF (present/absent), the degree of FF fibrosis (grades 1, 2 or 3), myxoid changes in FF, mitotic activity index (MAI) and sTILs%). ER, PR and HER2 were assessed using IHC for the purpose of this study with adequate quality controls.35 For 23 cases, only biochemical data were available for ER and PR, for this purpose, all samples with a protein values less than 10 fmol/mg were labelled negative. JPAB performed a blinded reproducibility analysis of FF and sTILs.
The grade and histological type were evaluated according to the WHO 2019 classification36 and divided into two groups: invasive breast carcinoma of no special type (NST) and others. FF was defined as the presence of proliferated fibroblasts and/or collagen fibres in varying proportions, as being larger than 1 mm and surrounded by carcinoma.25 Additionally, the degree of fibrosis in FF is classified into three groups according to the following criteria: Grade 1 FF consists of a large number of fibroblasts with a small number of collagen fibres (figure 1a); grade 3 FF is mainly composed of collagen fibres, mostly hyalinised (figure 1b) and grade 2 is intermediate between grades 1 and 3.22 25 The MAI was assessed according to the WHO classification by counting mitoses in 10 high-power fields with a field diameter of 0.42 mm for tumour grading and reporting the mitotic count per mm.2 36 37 This study used different prognostic thresholds for the MAI to form three groups: <3 vs ≥3 (MAI3), <5 vs ≥5 (MAI5) and <10 vs ≥10 (MAI10). TILs were evaluated in H&E-stained sections according to TIL-WG guidelines.8 The evaluation focused on lymphocytes and plasma cells and excluded necrosis, polymorphonuclear cells and tertiary lymphoid structures. Depending on the localisation of TILs, they were categorised as sTILs, located between tumour nests and along the invasive margin of the tumour or intratumoural TILs, which are very rare and directly interacting with tumour cells. This study scored the number of sTILs in each case as a continuous variable (figure 1c, d).8 We studied different prognostic sTILs values: 40% (two-tier, sTILs40), a three-tier partition (0%–5%, 6%–30% and 31%–100%), a four-tier partition (0%–5%, 6%–10%, 11%–40% and 41%–100%), and 10th percentile thresholds (10%, 20%, …80%, 90%). Tumour size and LN status were obtained from the pathology report.

Fibrotic focus (FF) is an easily detectable stromal feature in the centre of the tumour, Grade 1 FF (H&E×40) (a) and Grade 3 FF (H&E×40) (b). Stromal tumour-infiltrating lymphocytes (sTILs) are in stromal areas between tumour nests, low (<40%) (c) and high (≥40%) sTILs (d) (H&E×200).
Survival endpoints
For survival analyses, both overall survival (OS) and distant metastasis-free survival (DMFS) were the endpoints. In the analyses for OS, we defined the patients as alive (n=125) or death (n=106) at the last follow-up visit. In the analyses for DMFS, we defined distant metastases as any recurrence at a distant site or death from TNBC (n=82). All other patients were censored from the date of the last follow-up visit as being alive and well (n=149) or as death from causes other than BC (n=33) and local or regional recurrence (n=5).
Statistical analysis
Statistical analyses were conducted using SPSS (V.26.0; IBM SPSS Statistics) and MedCalc (V.22, MedCalc, Ostend, Belgium). Additionally, receiver operating characteristic (ROC) curve analysis, medians, tertiles, quartiles and 10th percentiles were used to establish the optimal prognostic thresholds of continuous variables. Kaplan-Meier survival analysis was used. Cox regression analysis yielded the relative importance of potential prognostic factors, which are reported as HRs with 95% CIs and beta values. An independent samples t-test determined group differences. Pearson’s χ2 test revealed the relationship between grouped variables. The Pearson correlation coefficient (r coefficient) test was used to determine the agreement between continuous variables that were normally distributed. A probability of rejecting or failing to reject the null hypothesis (p value) of <0.05 was regarded as statistically significant. Beta values were used to derive a multivariate prognostic TNBC index for each patient. Classification and regression tree (CART) analysis was used to design a prognostic decision tree. CART recursively partitions observations in a dataset into progressively smaller groups.
Results
Median follow-up was 128 (4–383) months and a total of 106 out of 231 TNBC patients died (45.9%). 82/231 TNBC patients (35.5%) developed distant metastases, and for 7%, this occurred between 8 and 31 years. Furthermore, 199 (86%) of the TNBCs were NST subtype and 107 (46.3%) were LN-positive patients. The median tumour size, MAI and sTILs were 2.20 cm (range: 0.1–10 cm), 14 mitoses per mm2 (range: 0–131) and 10% (range: 1–99%), respectively. FF occurred in 102 patients (44.2%) and 76 (75%) patients had grade 3 fibrosis. In the reevaluation of FF, both researchers reached exactly the same result with 100% agreement. FF correlated significantly with MAI5 (p=0.0002) and grade (p=0.02) but not with sTILs40, tumour diameter, LN status or age50. While sTILs did not exhibit any significant correlation with any other variables.
Prognostic Kaplan-Meier survival evaluation of different sTILs percentile thresholds (table 1) and ROC curve analysis showed that the optimal prognostic decision threshold was 40%. Patients with <40% sTILs showed worse survival (60.2%) than those with ≥40% sTILs (76.7%) (p=0.03). The three-tier (0%–5%, 6%–30% and 31%–100%) and four-tier (0%–5%, 6%–10%, 11%–40% and 41%–100%) partitions were not significant (p=0.14 and p=0.22, respectively). After the reevaluation of 17 samples with sTILs, there is a strong, statistically significant positive correlation (r=0.838, p<0.0001) between two researchers.
Prognostic evaluation of two-tier thresholds of sTILs in the 231 TNBC patients
MAI5 had the lowest probability of no differences among all the MAI thresholds (table 2). MAI3 and MAI5 thresholds were highly sensitive and had high negative predictive value, but the MAI5 threshold showed slightly higher specificity and a slightly better percent correct score than MAI3. The negative predictive value of MAI5 was higher than that of MAI10. Therefore, MAI5 is the most suitable threshold for further analyses.
Summary of MAI3, MAI5 and MAI10 performance metrics
The univariate survival and HRs of all characteristics for DMFS are shown in table 3 and for OS are shown in online supplemental table S1. Since DMFS provided more cancer-specific results than OS, DMFS was used in following analyses. Low-intermediate grade versus grade 3 (p=0.01), LN status (p=0.0002), the MAI (two different thresholds: p=0.007 and p=0.001), sTILs40 (p=0.03) and FF (p=0.0009) were significant univariate outcome predictors. None of the other characteristics were significant.
Supplemental material
Distant metastasis-free survival and HRs of all characteristics in the 231 TNBC
The multivariate survival Cox analysis that included all significant univariable features revealed that LN status was prognostically strongest (HR 2.07, 95% CI 1.32 to 3.23, p=0.0003), followed by FF (p=0.002), MAI5 (p=0.009) and sTILs40 (p=0.003) (p<0.0001) (table 4). Other features were not significant.
Multivariate Cox regression analysis (stepwise model) of the most significant features, χ2=34.8, p<0.0001
These four prognostic factors were used to construct a prognostic CART and a prognostic TNBC index for each patient; the patients were then arranged by decreasing index values (LN status 1=negative, 2=positive; FF 1=absent, 2=present; MAI5 1=<5, 2=≥5; sTILs40 1=<40, 2=≥40):
TNBC index=(LN status×0.73)+(FF×0.43)+(MAI5×1.57)+(sTILs40×−0.72).
ROC curve analysis, medians, tertiles and quartiles (online supplemental figure S1), and the coordinates of the curve (online supplemental table S2) were used to determine the optimal prognostic cut-off values for the TNBC index. With the ROC curve, the optimal threshold for distant metastases development was 3.80. Figure 2 shows the Kaplan-Meier survival curves reflecting the division of patients into tertiles based on the TNBC prognostic index (low: <3.58, n=64; intermediate: 3.58–4.01, n=87; high: ≥4.02, n=80) (p<0.0001) and HRs between the groups. Chemotherapy improved prognosis only in the high TNBC index group (p=0.05).

Survival curves of patients arranged in three groups according to the TNBC index score. TNBC, triple-negative breast cancer.
When LN status was excluded from the multivariate analysis, the same histopathological features were significant (p<0.0001): FF (HR 1.63, 95% CI 1.04 to 2.56, p=0.001), MAI5 (p=0.003) and sTILs40 (p=0.009). Other features were not significant.
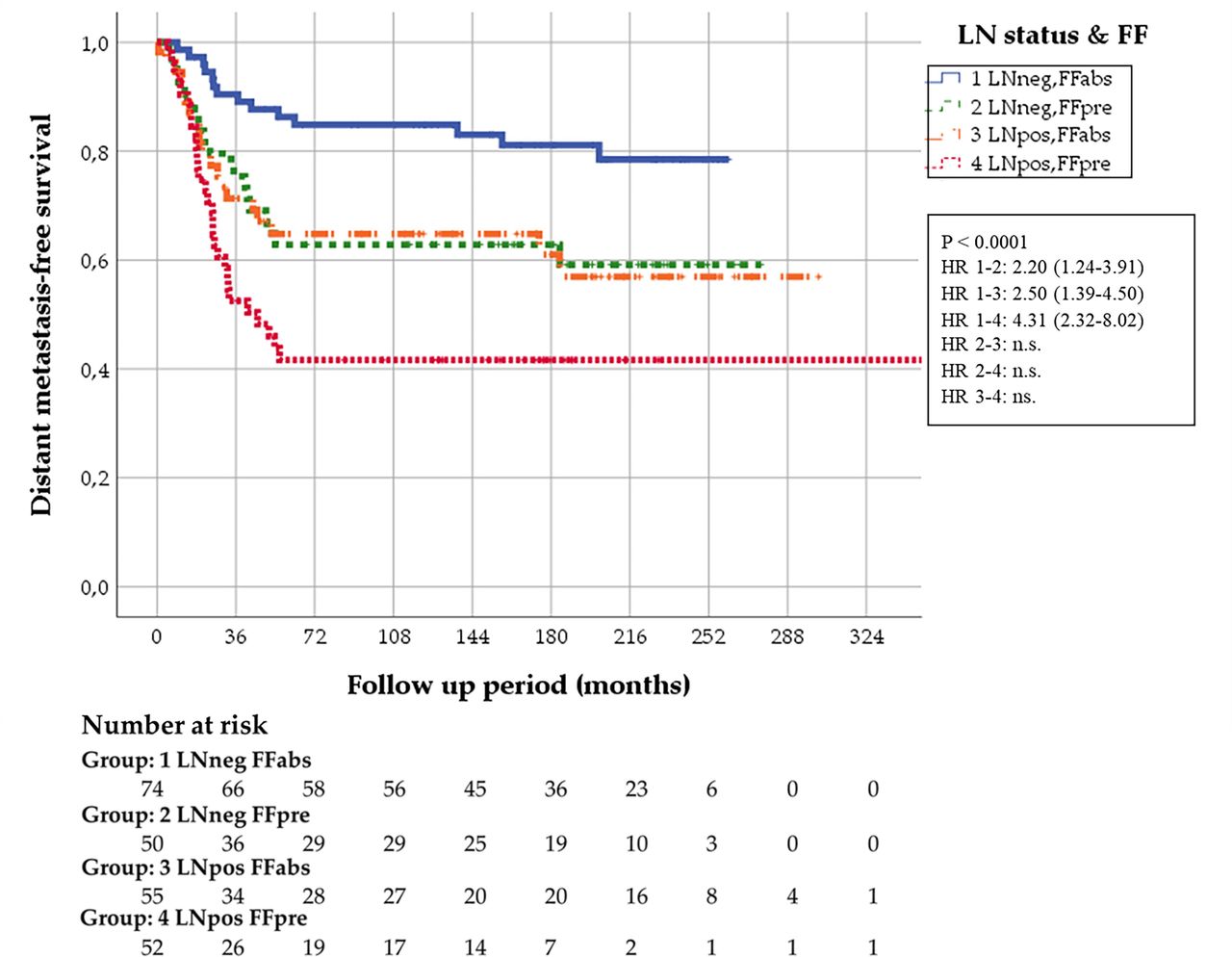
FF presence was associated with worse survival in TNBC (p=0.0009), both in LN-negative (p=0.02) and LN-positive (p=0.06) patients and in patients aged <50 and ≥50 (both p=0.02). Even in the small group of 20 LN-negative patients with MAI<5, FF presence was significant (p=0.02), but the number of FF-present cases was very small (n=2). Figures 3 and 4 show the survival curves for the four different subgroup combinations of LN status, FF and MAI5.

Survival curves of the four different subgroup combinations of LN status and FF. FF, fibrotic focus; LN, lymph node.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Survival curves of the four different subgroup combinations of LN status and MAI5. LN, lymph node; MAI, mitotic activity index.
The prognostic classification tree showed that patients with ≥40% sTILs showed better survival than <40% sTILs (survival rates of 78% and 60%, p=0.03). sTILs40 was associated with better survival in patients with MAI≥5 (p=0.06) but not in those with MAI<5 (p=0.49). Among the 94 LN-positive patients with MAI≥5, sTILs40 was a significant prognostic marker (p=0.05), with ≥40% sTILs (survival rate of 68%, n=25) improving survival in this unfavourable group (45% survival rate for <40% sTILs).
Within the 131 patients who underwent adjuvant chemotherapy (ACT), sTILs40 (p=0.03) and FF (p=0.02) were prognostic factors and interestingly, LN status, MAI5 and grade of tumours were not significant. In those patients who did NOT receive ACT, LN status (p=0.002), FF (p=0.009), MAI5 (p=0.001) and low grade (grade 1–2 versus 3) (p=0.004) were significant. ACT improved survival only in LN-positive patients (p=0.04) and in the patients with LN-positive and MAI≥5 (n=87, p=0.046).
Discussion
TNBC patients are often younger, and TNBC tumours show considerably higher proliferation than non-TNBC tumours, except for low-grade rare TNBC subtypes.6 Although one study has shown that low-grade TNBC had better prognosis,6 we could not demonstrate this relationship due to the small number of patients in this subgroup (n=13). However, we observed a similar result when the low-grade and intermediate-grade groups were combined. This study showed the importance of very long follow-up: 7% of distant metastases occurred after 8 years of follow-up. Most of the TNBC studies had short follow-up and they included few patients, except one.33
LN status, FF, sTILs40, MAI3, MAI5 and grade (1–2 versus 3) had univariate prognostic DMFS value, but the other characteristics did not. With multivariate analysis, FF, MAI5 and sTILs40 were significant alongside LN status. Based on the multivariate prognostic TNBC index, two groups of patients were clearly distinguishable; the low-index group (n=64, 28% of all cases, 10-year survival of 88%) had a very good prognosis, whereas the high-index group had an extremely poor prognosis (10-year survival of 44%), but all distant metastases occurred within 7 years. Patients in the intermediate-index group had a 34% risk of distant metastases and should be considered clinically high-risk patients. This is consistent with the malignant nature of TNBC. Although it provided very promising results, the prognostic TNBC index requires further validation.
We confirmed that FF presence is an independent DMFS prognostic factor in TNBC.24 32 33 A new finding of the current study is that it is prognostically significant in LN-negative patients under and above 50 years of age, respectively. This is in agreement with previous studies on LN-negative, non-TNBC patients under 55 years.21 38 This study also found that FF has additional prognostic value alongside the LN status. Moreover, FF presence is strongly related to high MAI values. Therefore, a practical implication for pathology laboratories is to reanalyse the MAI in TNBC cases with a low MAI and FF present. FF has an advantage over MAI determinations: FF is easy to assess and very reproducible. Although in the previous non-TNBC study, the cut-off value for age was 55,39 in the present study on TNBC, the age threshold of 50 appeared to be the appropriate cut-off value, as it is a better proxy for pre–post menopausal status. Although our current study observed a higher incidence of grade 3 fibrosis than grade 1, a previous study found that luminal subtypes, particularly luminal B, predominantly exhibited grade 3 fibrosis.40 That study only included 24 TNBC patients and 10 of these had grade 3 fibrosis. As such, it seems that grade 3 fibrosis is very much correlated to the rate of proliferation, as previously also observed.21
The fact that the median for the MAI in TNBC was high (14 per mm2) and that MAI5 was much significantly prognostically stronger than MAI10 (the optimal threshold for other molecular BC phenotypes) showed again how aggressive TNBC is. It is known that low-grade TNBCs are less aggressive and show lower MAI.6 Our study confirmed this, even though this subgroup included only a small number of patients. This means that there are many more dormant distant metastases in TNBC than in non-TNBC, which grow even with low proliferation rates to become clinically evident distant metastases. Moreover, in TNBC patients with MAI<5 (low proliferation), both LN-negatives and LN-positives had favourable survival, whereas patients with MAI≥5 had an unfavourable prognosis regardless of LN status. This shows the dominant prognostic effect of MAI≥5 over LN status in TNBC. Large, multicentre studies have shown that protocolised MAI assessments demonstrated strong intra and interobserver reproducibility39 and very strong prognostic value,29 much stronger than subjective non-quantitative mitotic impressions.41
Regarding the more prominent sTILs in TNBC, the immunosurveillance theory suggests that TNBC may harbour tumour variants that are highly antigenic, thus making it better able to trigger a host’s immune system to mount an antitumour response. Other studies showed that sTILs are not a prognostic factor in luminal subtypes, in contrast with TNBC.12 42 The results of the present study are in agreement with a meta-analysis that found that a high level of sTILs is prognostically favourable,43 similar to the results of other studies.14–18 42 44 45 The two-tier sTILs40 method has the most optimal sensitivity and specificity and may improve observer reproducibility.46 Future quantitative and unbiased assessments of sTILs are crucial. The use of artificial intelligence (AI) will help increase the reproducibility of the assessments; such analyses should, of course, need a new threshold evaluation. The results of a semiautomated quantitation study showed that it can be just as reproducible as fully automated digital assessment but is more time-consuming and sensitive to interobserver variability.47 Therefore, the development of a rapid and well-reproducible quantification method is required. FF was highly reproducible; however, sTILs evaluation could be improved to enhance reproducibility.8 A grid-point approach in standard image analysis and digital algorithms based on AI (deep learning and machine learning) using different platforms has potential in the development of such a method,48–53 and further studies are ongoing. This would contribute to more consistent and reliable assessments for sTILs. Additionally, the FDA developed a continuing medical education course and made it available globally to train pathologists in assessing sTILs in H&E slides. Such efforts will improve the expertise of pathologists participating in assessing and reporting sTILs in clinical trials.54
Recently, a large retrospective study was published with long follow-up, including young (<40 years old) chemotherapy-naïve LN-negative TNBC patients mostly.33 Studying BC-specific survival, they reported that sTILs with a 30% cut-off was a strong prognosticator with LVI and FF having additional prognostic value. Unfortunately, in our cohort, we only had five chemotherapy-naïve young patients and as such, we were not able to confirm their results exactly. In our older chemo-naïve population (n=74), which included both LN-negative (n=53) and LN-positive (n=21) patients, those with high sTILs40 (≥40%) had a better DMFS; however, due to the limited number of cases the results were not significant (online supplemental figure S2).
One limitation of the study was that the H&E slides were prepared from older paraffin blocks, with some cases requiring re-embedding in new paraffin blocks for sectioning. Additionally, a portion of the ER and PR results (n=23), particularly for older cases, was obtained through biochemical staining methods. For all other cases where ER, PR and HER2 markers were not assessed at diagnosis, new sections were obtained and subjected to IHC and evaluated according to quality control criteria. Finally, the ACT administered to patients may have varied over the years, as the Norwegian treatment guidelines have evolved in terms of agents and dosing frequency over time. This variability should be considered when interpreting the ACT effect analysis results.
In conclusion, FF, MAI and sTILs constitute the strongest independent prognostic set of histopathological features in TNBC with long follow-up. The MAI and FF are well reproducible. The presence of FF in TNBCs with MAI<5 requires repeated MAI assessment. sTILs40 has prognostic value, but the development of a quantitative determination method that is unbiased and automated is essential. The multivariate prognostic TNBC index provides information on the probability of low and high distant metastases in different subgroups.
Data availability statement
Data are available on reasonable request. The dataset generated during the current study is not publicly available because of ethical and legal concerns. Anonymised data can be made available from the Stavanger University Hospital Institutional Data Access/ Ethics Committee (contact via email: rek-vest@uib.no, REK vest, Rogaland, Vestland, Norway) for researchers who meet the criteria for access to confidential data.
Ethics statements
Patient consent for publication
Ethics approval
The Norwegian Regional Committee for Medical and Health Research Ethics (REC, 2010/1241) approved this study. REC approval meant that the need for informed consent was not required as the tissue samples had already been removed for diagnostic and treatment purposes.
Acknowledgments
The authors would like to thank Jan P. A. Baak for his valuable help with the statistical analyses.
References
Footnotes
Handling editor L C Collins.
Contributors Conceptualisation, UK and EAMJ; data curation, UK, ER, KBP, DMA and SHR; formal analysis, UK, EGG, JPAB and EAMJ; methodology, UK and EAMJ; supervision, JPAB and EAMJ; writing-original draft, UK; guarantor, UK. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Funding This work was funded by the Horizon 2020 European Union research and innovation programme under the Marie Sklodowska Curie grant agreement No 860627 (CLARIFY Project).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.